Impact of Sedation and Echocardiographic Guidance Strategy on Left Atrial Appendage Closure
Purpose: Traditionally, left atrial appendage closure (LAAC) has been performed under general anesthesia (GA) with transesophageal echocardiography (TEE), but operators are increasingly utilizing conscious sedation (CS) or monitored anesthesia care (MAC) with intracardiac echocardiography (ICE). This study sought to assess the impact of sedation and echocardiographic guidance strategies (CS/ICE, MAC/ICE, GA/TEE, GA/ICE, and GA/TEE/ICE) on the procedural efficiency, outcomes, and safety of LAAC.
Material and Methods: This single center retrospective study included all patients who underwent LAAC with Watchman FLX from June 2021 to November 2022. Primary measures were patient in-lab, sedation start, device release, vascular closure, and patient out-of-lab times. Secondary measures were successful transseptal puncture, successful device deployment, number of deployed devices, fluoroscopy time, contrast volume, length of stay, complications, and incidence of peri-device leak and device-related thrombus at follow-up.
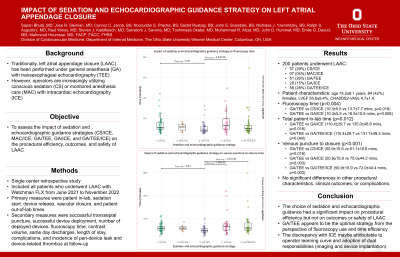
Results: 200 patients underwent LAAC. 57 (29%), 7 (4%), 51 (26%), 29 (15%), and 56 (28%) with CS/ICE, MAC/ICE, GA/TEE, GA/ICE, and GA/TEE/ICE respectively. Patient characteristics were notable for age 75.2±8.1 years, 84 (42%) females, LVEF 55.6±9.4%, and CHA2DS2-VASc 4.7±1.4, with no difference between groups. There was a significant difference among groups in fluoroscopy time (p=0.004), specifically with GA/TEE vs CS/ICE (10.3±5.5 vs 13.7±7.7 mins, p=0.016) and GA/TEE vs GA/ICE (10.3±5.5 vs 16.5±10.5 mins, p=0.006). There was a significant difference among groups in the total patient in-lab time (p=0.012), specifically with GA/TEE vs GA/ICE (110.4±29.7 vs 135.0±48.6 mins, p=0.016) and GA/TEE vs GA/TEE/ICE (110.4±29.7 vs 131.7±49.3 mins, p=0.040). There was a significant difference among groups in the time from venous puncture to closure (p < 0.001), specifically with GA/TEE vs CS/ICE (50.9±15.9 vs 61.1±18.6 mins, p=0.016), GA/TEE vs GA/ICE (50.9±15.9 vs 75.0±44.2 mins, p=0.003), and GA/TEE vs GA/TEE/ICE (50.9±15.9 vs 72.0±44.4 mins, p=0.003). There were no significant differences in other procedural characteristics, clinical outcomes, or complications.
Conclusions: The choice of sedation and echocardiographic guidance had a significant impact on procedural efficiency but not on outcomes or safety of LAAC. GA/TEE appears to be the optimal strategy from the perspective of fluoroscopy use and time efficiency.