Racial Differences in Device-Detected Incident Atrial Fibrillation
Purpose: Prior research suggests that Black individuals have a higher prevalence of cardiovascular risk factors, but lower risk of atrial fibrillation (AF) than White individuals. Whether this paradox persists utilizing highly sensitive methods of AF diagnosis has not been well studied. This study aimed to compare the incidence of device-detected AF between Black and White individuals with a cardiac implantable electronic device (CIED).
Material and Methods: A retrospective analysis of patients > 18 years old with no history of AF who had a Medtronic CIED implanted in the United States between 01/01/2007 - 06/01/2019 was conducted. Patients with insertable cardiac monitors, and insufficient remote monitoring were excluded. The primary endpoint was time to first device-detected AF. Cox proportional hazards modelling was used to compare differences in incident AF between Black and White individuals.
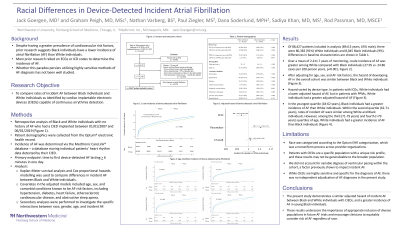
Results: Of 441,047 patients with a Medtronic CIED, 88,427 patients (mean age 69 + 13 years, 80,382 (91%) White, 55,840 (63%) male) were included in analysis. There were 35,143 individuals (40%) with device-detected AF. Over a mean of 2.2±1.7 years, crude incidence of AF was greater among White compared with Black individuals (27.95 vs. 24.86 cases per 100 person years, p< 0.001). After adjusting for age, sex, and AF risk factors, the hazard of developing AF in the overall cohort was similar between Black and White individuals (HR = 1.02, 95% CI: 0.98-1.06). Hazard varied by device type whereby among those with ICDs, White individuals had a lower adjusted hazard of AF (HR=0.93, 95% CI: 0.89-0.98), but among those with PPMs, White individuals had a greater adjusted hazard of AF (HR=1.11, 95% CI: 1.03-1.19).
Conclusions: White individuals had a higher crude incidence of device-detected AF, however, after controlling for age, sex and AF risk factors, the hazard of developing AF was similar between Black and White individuals. These results challenge the notion that Black individuals are at lower risk of developing AF than White individuals and encourage clinicians to equitably consider risk of AF in patients of both races.